The Inversion
TL;DR
The flight is at 6 a.m. The man across the aisle is in his late fifties. He stands to pull his bag from the overhead bin, and his whole body argues with the motion. He gets the bag down. It costs him three seconds and a wince he tries to hide. He is at the peak of his career and the bottom of his physical reserve, in the same airport, on the same morning.
That's the inversion.
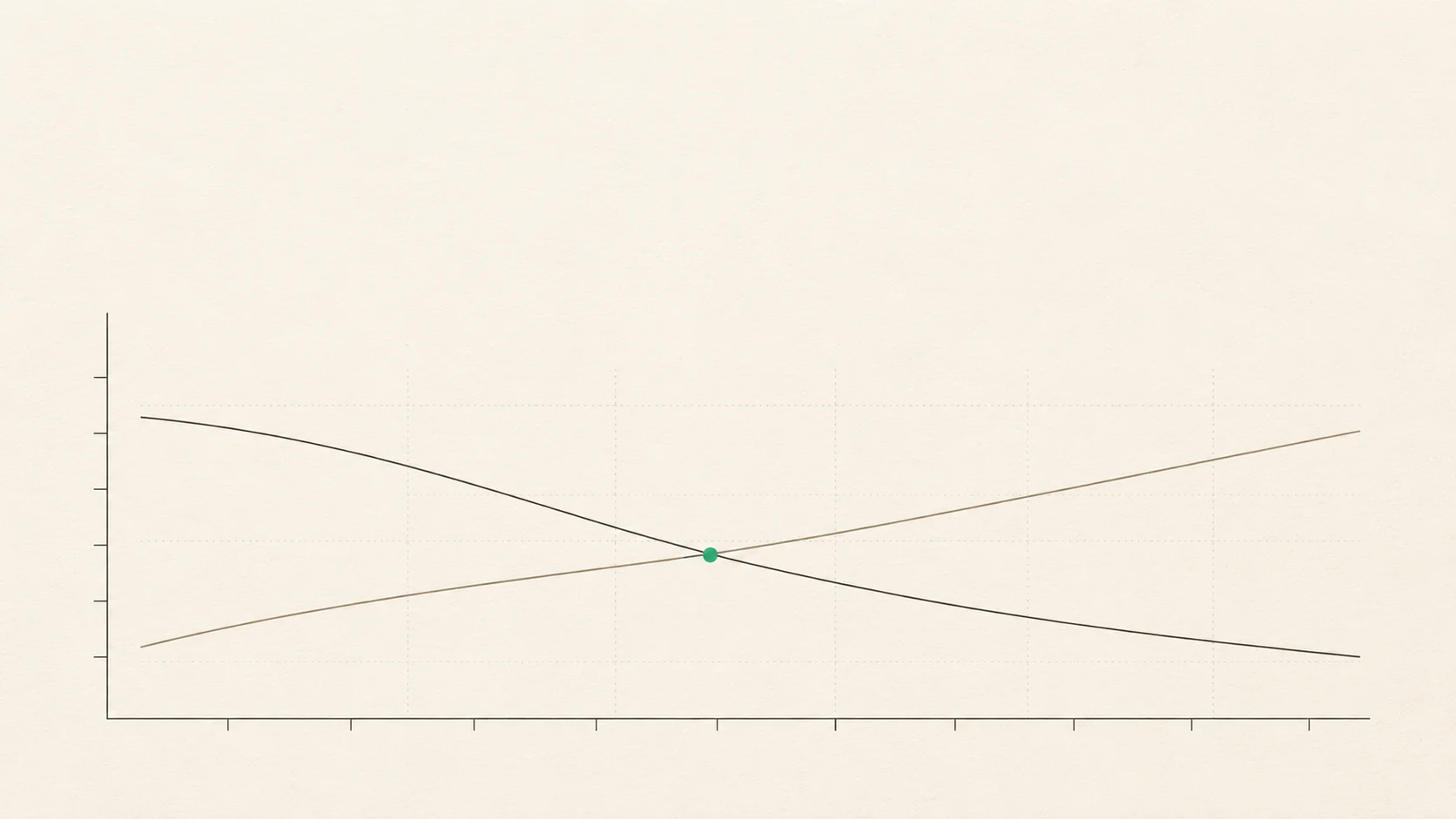
Career leverage for high performers peaks in the mid-fifties. Muscle strength starts declining at thirty-five. By the time you can finally spend the harvest, you've run an unmanaged physical system for twenty years without a single measurement.
Two curves moving in opposite directions, and almost nobody does the math on both.
You have spreadsheets for your 401(k). Quarterly reviews, projection models, rebalancing rules, a target date, a fiduciary who calls you the moment anything drifts. Your financial system is instrumented. You'd fire a manager who ran a department the way you run your body. Now ask what the equivalent system looks like for the only asset that has to show up at sixty-five to spend the money.
The Math You Haven't Done On Your Body
Start with the numbers. They're worse than most people guess. How bad depends entirely on when you start.
Aerobic capacity, measured as VO2max, drops about 10 percent per decade from your mid-twenties onward in sedentary adults (Jackson et al., Astrand). That's the fuel tank. By fifty a quarter of it has drained, and nobody told you, because the dashboard the medical system hands you has no gauge for it.
Muscle strength starts its measurable decline at thirty-five. Without resistance training, adults lose 3 to 8 percent of muscle per decade through midlife, and the rate speeds up after fifty (Janssen et al., Frontera et al.). Sarcopenia doesn't get diagnosed until it's clinical, which is two decades after it started.
Cognitive processing speed begins slipping around forty-five in population data from the Whitehall II cohort (Singh-Manoux et al., BMJ 2012). That's a finding about aggregates, not a verdict on any one person, and it's softer than the physical numbers. The direction is the same, though. The things you lean on at work start drifting before the chart shows anything.
So here's where it lands. You're managing a Body 401(k), and the early withdrawals happen whether you watch or not. Aerobic capacity, muscle, balance, speed of movement, speed of thought. Every decade you skip a deposit, you draw down the principal you'd need at seventy to fund the life you're picturing at fifty-five. The account exists. The contributions don't.
You cannot make up twenty years of missed contributions at age seventy. That's the mechanical fact. Your plasticity is highest right now, in this decade, and the window narrows every year you wait.
The Measurement System That Can't See You
Your annual physical checks for disease. That's what it's for, and it does that job well enough.
But disease is not capacity. The lipid panel doesn't know whether you can still get off the floor without using your hands. The blood pressure cuff has nothing to say about whether your grip strength has dropped 15% since forty. The 15-minute visit gets billed against a list of CPT codes, and capacity isn't on the list. So the room you're paying to sit in has no instrument that could see the thing most likely to decide what the next thirty years actually feel like.
The healthspan-lifespan gap in the US is 12.4 years, the largest in the world (Garmany et al., JAMA Network Open, 2024). Twelve years where you're alive but your body has already stopped letting you do the things that made the life worth living. Musculoskeletal decline is one of the primary drivers of that gap, and it's the one the system is worst at catching early.
This is the part that should embarrass anyone who runs a business. You have dashboards on customer churn that flag a 3% drift inside a week. You have a dashboard on your body that wouldn't flag a 30% drift across a decade. A department head with metrics that bad would have been gone two quarters ago.
The issue is structural. The US system is a reactive apparatus by design. Revenue is keyed to diagnosis and procedure. Nothing in the codebase rewards catching a functional decline in year three of a twenty-year drift. Sitting inside that system, you're left with a dashboard that lights up only when the house is already on fire.
You can't fix the system. You can install your own dashboard.
The Compounding Window
Here's why this decade matters more than the next one.
Taina Rantanen and colleagues measured midlife grip strength in Japanese-American men and followed them for 25 years. Higher midlife strength meant lower late-life disability, and the relationship was dose-dependent (Rantanen et al., JAMA 1999). What you banked at fifty paid out at seventy-five, and it paid out as measurable independence: walking, carrying, getting up and down, staying out of assisted living.
The InCHIANTI study, run out of Tuscany by Ferrucci and the NIA, tracked a broader European cohort and found the same pattern. Midlife physical activity predicted late-life mobility independent of age, sex, and baseline health. What got put in during the forties and fifties was still paying out decades later. Call it what it is. Compounding, as real for a body as it is for an index fund.
The reversibility data is the part the "it's too late at fifty" voice in your head needs to hear. Resistance training studies in adults 50 to 65 show 10 to 46 percent strength gains depending on the protocol and the muscle group (Peterson et al., American Journal of Medicine, 2011). VO2max studies in the same age band show 15 to 25 percent gains over twelve weeks (Wisløff et al., Circulation, 2007). The plasticity gap between fifty and eighty is enormous. The door closes slowly, not suddenly, and at your age it's still wide open.
So you're not behind on the biology. You're behind on the inputs. Two diagnoses. Only one is fixable, and it's the one you've got.
Every year you wait, the slope of reversibility flattens. Every year you start, the dividend pays out across more of the remaining decades. This is why the numbers on the retest matter more than the number on the baseline. You're reading a rate of change, not a verdict.
What It Actually Costs To Skip This Window
The Cleveland Clinic group led by Mandsager ran treadmill tests on 122,007 adults and watched the mortality data for a decade. Adults in the bottom twenty percent of cardiorespiratory fitness had a hazard ratio of 5.04 for all-cause mortality versus elite fit adults (Mandsager et al., JAMA Network Open, 2018). That effect size is comparable to or greater than traditional risk factors including smoking.
Take that in as scale, not as fear. A 5x multiplier on mortality is what you're trading away when the maintenance budget stays at zero for another decade. The bill never arrives in the mail. It gets paid on the back end, drawn from the years you assumed you'd have and then didn't.
Here's the reframe that matters. The biology is still responsive. The plasticity is still there. What's missing is an operational framework, a measurement cadence, and a contribution system that runs on autopilot, not on willpower.
Look at the master athletes in their seventies. Look at the fifty-year-olds who started at forty-eight and are stronger now than they were at thirty-five. The data doesn't say the window closes. It says the window gets narrower, slowly, and the returns are highest on the contributions made inside it.
This is the window. You're in it right now.
Your First Audit, Ten Minutes, No Equipment
Here's the deposit. Tonight. Ten minutes. No equipment.
Test 1: Five-times sit-to-stand, timed. Standard chair, arms crossed over your chest. Stand up, sit down, five full reps, as fast as you can do it safely. Under seven seconds is good at most ages. Over twelve is a signal. Write the time down.
Test 2: Single-leg balance, eyes closed, thirty seconds. Bare feet, arms free, stand on one leg, close your eyes, count the seconds until you put the other foot down or open your eyes. Thirty seconds is the ceiling. Under ten is a signal. Do both legs and record the worse one.
Test 3: One loaded carry across the room. A kettlebell, a dumbbell, a packed duffel, anything in the 25 to 50 pound range. Hold it in one hand at your side. Walk across the room with a straight spine and no list toward the loaded side. Switch hands. Walk back. Note whether your grip or your back gave first, and how it felt.
Write all three numbers down. That's the baseline. Those are your first receipts.
Retest in six weeks. Not six months. Six weeks is long enough for the training to produce a readable signal and short enough that you'll still remember why you started. If the numbers moved, the system works. If they didn't, your input needs to change, and now you have the data to know that before another year goes by in the dark.
Build one worst-week-proof habit around the three tests. Something that runs on your worst week, not your ideal one. Ten sit-to-stands a day. Two minutes of single-leg balance while you brush your teeth. One loaded carry on the way from the car to the door. The floor is low on purpose, because the floor is what survives the weeks that break every other plan.
TL;DR
- Career leverage peaks in the mid-fifties. Muscle strength starts declining at thirty-five. That's the inversion.
- You manage a Body 401(k). Every decade without deposits is a drawdown from principal you'd need at seventy.
- Your annual physical checks for disease, not capacity. The healthspan-lifespan gap in the US is 12.4 years, and MSK decline is a primary driver.
- Midlife grip and activity predict late-life mobility 25 years later. The compounding is real, and the window is still open.
- Five-times sit-to-stand, 30-second single-leg balance, one loaded carry. Ten minutes tonight. Retest in six weeks.
FAQ
Is 50 too late to start? No, and the data is cleaner on this than you'd think. Resistance training in adults 50 to 65 produces 10 to 46 percent strength gains. VO2max studies in the same cohort show 15 to 25 percent gains over twelve weeks. The plasticity gap between 50 and 80 is real. You're not late. You're on time for a system you haven't built yet.
How often should I retest? Every six weeks for the first six months. Quarterly after that. Annual retesting hides the trend line, which is the only data that tells you whether your inputs are working.
Is this about longevity or capacity? Capacity. Longevity is a downstream effect of a body that stayed capable. The metric you manage is what you can still do. The years follow from the capability, not the other way around.
What if my doctor says I'm fine? Fine means no disease flagged. It doesn't mean your capacity is where it should be for the life you want in ten years. Disease is the wrong KPI for a system that's asymptomatic until it isn't. Your doctor is doing the job they were trained for. You need a different job done, and you're the one who has to commission it.
Which metric matters most if I only pick one? Grip strength, if you want a single number that predicts a lot, because it loads onto whole-body strength, neuromuscular integrity, and cardiovascular risk. If you can't get a dynamometer, use the five-times sit-to-stand. Either one, retested every six weeks, will tell you whether the system is working.
Book your Healthspan Snapshot, we'll run the capacity tests your annual physical doesn't.
Or book a Mapping Session if you want a full operating framework built around your baseline, your schedule, and the twenty-year plan you've been running without a dashboard.
This is a common pattern, not a diagnosis. If any test feels unsafe, stop. If pain is sharp, radiating, or accompanied by numbness, see a clinician before retesting.
Educational purposes only. Not medical advice, diagnosis, or treatment. Consult your qualified healthcare provider.
Ready to build capacity?